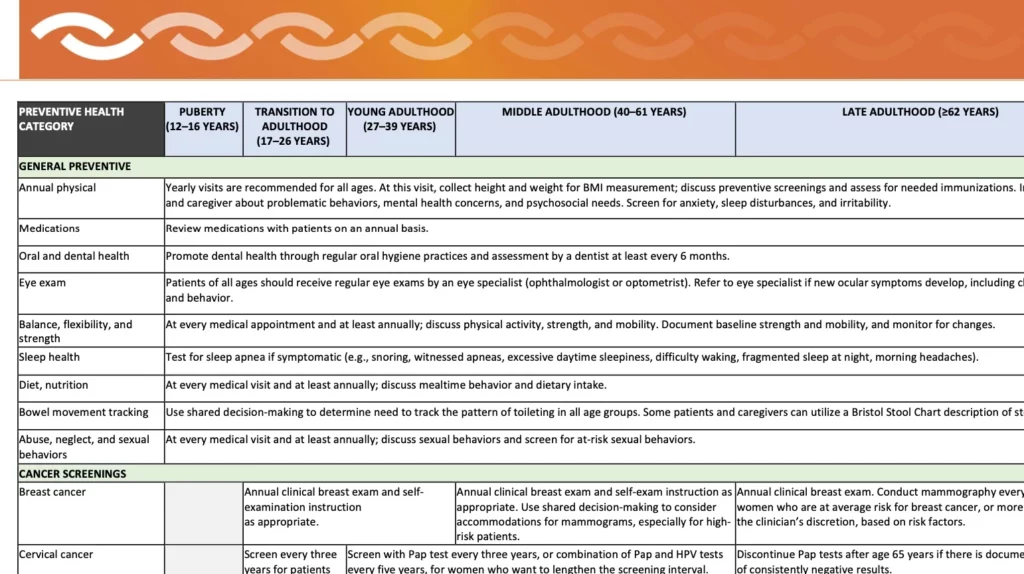
Staying healthy in middle age

Keeping up with life plans is key as autistic adults and caregivers reach maturity
Maintaining continuity while being prepared for changes
Make sure paperwork is up to date
Staying organized
Keeping benefits in place often requires an annual review
Updating health care documents
Check in with the family – adult siblings may need to understand how to be prepared.

Manageable moments
Meeting the challenges of midlife



Getting an autism diagnosis as an adult
Women and Autism
This Q & A is based on a LurieNOW article by Dr. Alyssa Milot Travers, a licensed psychologist at the MGH Lurie Center for Autism with specific expertise in women on the autism spectrum. Dr. Travers is also an Instructor in Psychiatry at Harvard Medical School.
How prevalent is autism?
Is ASD underdiagnosed in women?
Recognizing the uniqueness of each autistic individual's experience, what other traits may be more common in women with autism?
So is there a detriment to masking and camouflaging? These behaviors are often viewed positively as coping skills by those not familiar with neurodiversity.
Many men with autism have special interests and repetitive behaviors — is this also true for women?
Restricted interests and repetitive behaviors occur in autistic men and women; however, the nature of these behaviors can differ. Traditionally, clinicians have been trained to recognize stereotypical male-associated restricted interests, such as transportation, dinosaurs, or space. In contrast, autistic women may develop restricted interests that are more closely aligned with societal norms, such as animals, art, celebrities, or literature.
This divergence can contribute to the misperception that women with these interests are simply showing enthusiasm for “normal” hobbies rather than autistic traits. Repetitive patterns of behavior in women can manifest as classic autistic behaviors like rocking or hand/finger movements, but may also appear as behaviors not necessarily associated with autism, such as perfectionistic tendencies or restrictive patterns of eating/eating disorders.
Are there co-occurring conditions that are more common in women?
Since some symptoms of autism may present differently in women, they may receive other diagnoses first, such as anxiety and mood disorders, learning disorders, and/or eating disorders. This phenomenon is called diagnostic overshadowing, which occurs when a person’s symptoms are attributed to a psychiatric problem versus an underlying medical issue or developmental delay such as autism. Such overshadowing can complicate the diagnostic process, as the focus may be on managing these secondary conditions rather than recognizing the underlying autistic traits.
What are some reasons a woman might seek an ASD diagnosis?
How does gender identity impact a woman seeking or receiving an autism diagnosis?
Most research about gender identity seems to focus on cisgender individuals, or those who have a gender identity matching their sex assigned at birth. When meeting with a provider, it is important to ask about their experience with women on the spectrum and how they tailor assessment methods and support for woman patients/clients. Women often benefit from woman-specific supports and resources.
Many individuals, including autistic persons, embody a range of gender identities, including but not limited to nonbinary and transgender. Recent research shows an increase in gender diversity within the autistic community compared to the population at large. Therefore, there has been a recent shift toward embracing gender diversity beyond the cisgender paradigm in research. Embracing an expanded understanding of what it means to be autistic will lead to a more inclusive perspective that ensures all individuals, regardless of gender, receive the recognition and support they deserve.
Where can I learn more?
The Autistic Women and Nonbinary Network provides useful information and resources for gender-diverse autistic individuals.
For diagnostic information, see our article about seeking an ASD diagnosis as an adult.
Recommended Reading and Viewing
For women:
Camouflage: The Hidden Lives of Autistic Women by Dr. Sarah Bargiela
22 Things a Woman with Asperger’s Syndrome Wants Her Partner to Know by Rudy Simone
The Autistic Brain: Exploring the Strengths of a Different Kind of Mind by Temple Grandin
Odd Girl Out: An Autistic Woman in a Neurotypical World by Laura James
From the American Autism Association: 5 TedX Talks from Women with Autism
For caregivers:
A Guide to Mental Health Issues in Girls and Young Women on the Autism Spectrum: Diagnosis, Intervention and Family Support by Dr. Judy Eaton
Girls Growing Up on the Autism Spectrum: What Parents and Professionals Should Know About the Pre-Teen and Teenage Years by Shana Nichols with Gina Marie Moravcik and Samara Pulver Tetenbaum
For partners of autistic adults:
Common Gastrointestinal Conditions in Autistic Adults
Autistic people are more likely to suffer from gastrointestinal (GI) ailments than the general population, but that doesn’t mean that recurring discomfort should be accepted as simply part of being autistic.
- Constipation
Constipation is the most common gastrointestinal complaint in autistic people and that’s true of the general population, too. For many people, constipation is a chronic health problem that can develop and persist at any point in the lifespan.
- Gastroesophageal Reflux Disease (GERD) and Acid Reflux
- Abdominal Pain
- Pica
Pica is a condition in which individuals with nutrient deficiency or some other process going on causes them to chew on or ingest non-food products. While present in the neurotypical population pica does appear more often in autistic people.



